|
<< Click to Display Table of Contents >> Functional/Cognitive Status |
  
|
|
<< Click to Display Table of Contents >> Functional/Cognitive Status |
|
A patient's Functional/Cognitive Status includes activities of daily living, cognitive, and disability status. To view the patient's Functional/Cognitive Status documentation, go to Patient Chart > Health History and see the entries under the Functional/Cognitive Status heading. Functional/Cognitive Status documentation will also display on the Patient Summary in the Function Status section. (TIP: Choose List View if you want to edit items in the list.)
This section covers the following topics:
To Document No Functional Impairments
To Document No Cognitive Impairments
To Add a New Functional/Cognitive Status Item
To Edit Functional/Cognitive Status Items
To Remove Functional/Cognitive Status Items
If the patient has no known functional impairments, it's important to document that. Select the No Known Functional Impairments option to note in the patient's record that there is no known functional impairments.
NOTE: Any new entry updated will overwrite the No Impairments entry.
If the patient has no known cognitive impairments, it's important to document that. Select the No Known Cognitive Impairments option to note in the patient's record that there is no known cognitive impairments.
NOTE: Any new entry updated will overwrite the No Impairments entry.
1.To add a new family health history item, go to Health History > New. The Health History Categories page is displayed.
2.Double-click Functional/Cognitive Status from the list of Health History categories. The Functional/Cognitive Status Search screen is displayed. A list of impairments and disabilities is displayed. The Type column displays whether the description is a Functional or Cognitive impairment.
3.Search for and locate the appropriate status by selecting the Description or SNOMED option in the drop-down list and then entering information into the Search field. Descriptions display in alphabetical order.
4.Double-click the desired impairment or disability (or select the desired impairment or disability and select Insert). The Functional/Cognitive Status Maintenance screen is displayed, and the Description, SNOMED code, Entered Date (current date), and Type are populated based on the item selected.
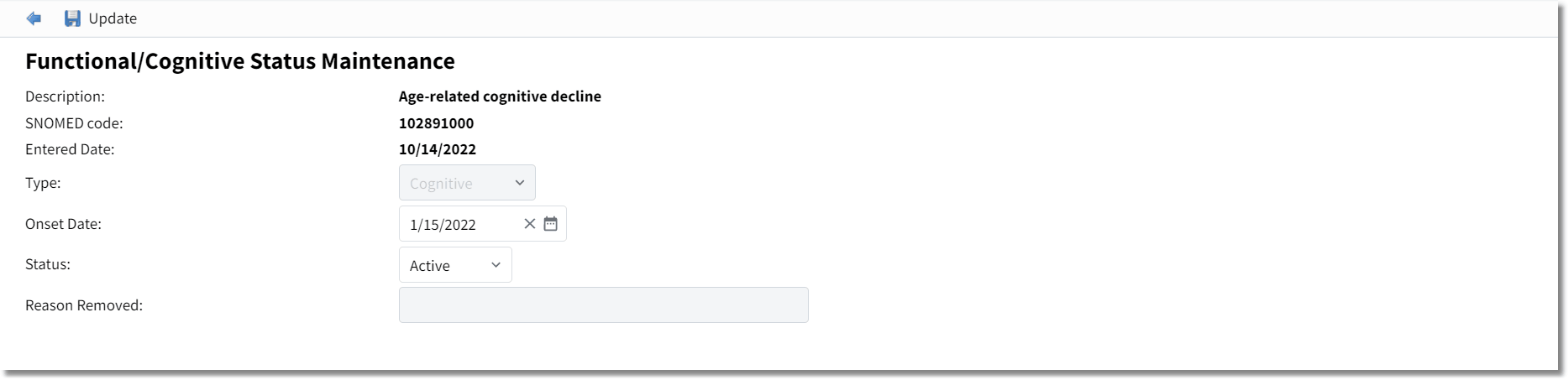
Functional/Cognitive Status Maintenance
5.Enter the Onset Date or select from the calendar.
6.In the Status field, select Active, Inactive, or Removed from the available drop-down. See To Remove Functional/Cognitive Status Items for additional details.
7.Select Update.
NOTE: If information is not saved, the system will prompt, "Are you sure you wish to exit without saving?"
1.Go to the Health History Review screen and select List View format.
2.Double-click the item to display the Functional/Cognitive Status Maintenance screen (or highlight the desired entry and select Edit).
3.Make the desired edits.
4.Select Update to save.
1.To remove a Functional/Cognitive Status item, go to the Health History Review screen and select List View format.
2.Double-click the item to display the Functional/Cognitive Status Maintenance screen (or, highlight the desired entry and select Edit).
3.In the Status field, select Removed. The Reason Removed field is enabled.
4.In the Reason Removed field, document the reason for removal (up to 50 characters).
5.Select Update to save the changes.