|
<< Click to Display Table of Contents >> Pertinent History |
  
|
|
<< Click to Display Table of Contents >> Pertinent History |
|
The Pertinent History section of the of the Initial Interview may include special coded questions that launch directly to an application, open a predefined answer or date box, and populate selected questions and answers to the 24 Hour Summary and Patient Summary reports. The majority of these questions display in red text when addressed on the flow chart. The exceptions are the inpatient arrival and questions and answers identified to print to the 24 Hour Summary and Patient Summary reports. Questions that display in red text will not display answer text in the date and time column on the flow chart. To view the information charted on these questions, select the question.
Special coded question include Inpatient Arrival Date/Time, Height and Weight, Smoking Status, Food Dislikes, Allergies, Home Medications, Family Health History, and questions set to print to the 24 Hour Summary and Patient Summary reports.
Inpatient Arrival Date/Time
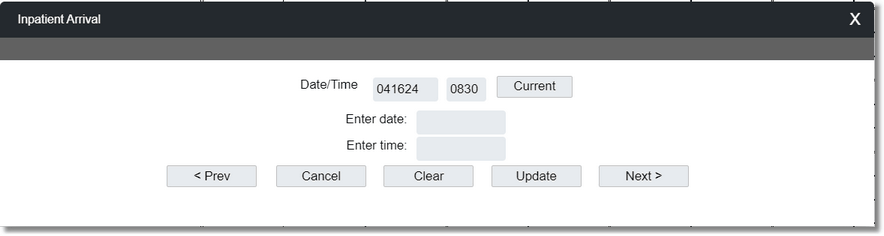
1. To document the date and time of the patient's arrival to the inpatient unit, select the Inpatient Arrival Date/Time question.
Inpatient Arrival Date/Time
2.In the Enter date field, enter the date of the patient's arrival to the inpatient unit in MMDDYY format.
3.In the Enter time field, enter the time of the patient's arrival to the inpatient unit in HHMM format.
4.Select Next to save the information and advance to the next question, Update to save the information and return to the flow chart, Clear to clear the entry, Cancel to clear the entry and return to the flow chart, or Prev to save the information and go to the previous question.
Height and Weight
1.To document the patient's admission height and weight, select the Height and Weight question. The Height/Weight section of the Vitals application displays for documentation.
NOTE: The patient's height and weight will display on the screen if previously documented in the Vitals application or if entered when the patient was admitted.

2.The Date/Time field defaults to the current date and time. Select Change Date/Time to modify the date and time.
3.In the Height /Length field, enter the height or length in inches or centimeters. The system will calculate the unentered value.
4.In the Weight field, enter the weight in pounds and ounces or kilograms and grams.
5.In the Scale field, use the drop-down to select the scale used.
NOTE: The BMI and BSA is calculated from the height and weight entered.
6.The BMI Not Measured field will be active if a height or weight is not entered. Use the drop-down and select the reason the BMI could not be measured.
7.In the Head Circumference field, enter the head circumference in centimeters or inches. The system will calculate the unentered value.
8.Select Update to save the information and return to the flow chart.
Smoking Status
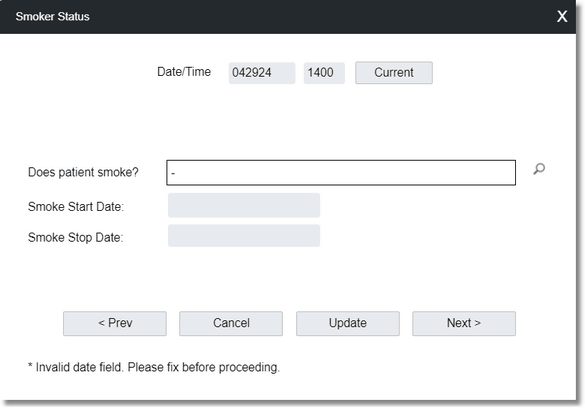
1.To document the patient's smoking status, select the Smoking Status question.
NOTE: The patient's smoking status will display on the screen if previously documented in Health History or if entered when the patient was admitted.
Smoker Status
2.The Date/Time fields default to the current date and time. Modify these fields, if necessary.
3.To the right of the Does patient smoke? field, select the lookup icon and select the patient's smoking status from the list.
4.In the Smoke Start Date field, enter the appropriate date in MMDDYYYY format, when applicable.
5.In the Smoke Stop Date field, enter the appropriate date in MMDDYYYY format, when applicable.
6.Select Next to save the information and advance to the next question, Update to save the information and return to the flow chart, Cancel to clear the entry and return to the flow chart, or Prev to save the information and go to the previous question.
NOTE: A patient's smoking status charted on this question will populate on the Social History-Tobacco/Nicotine Use screen in Health History.
Food Dislikes
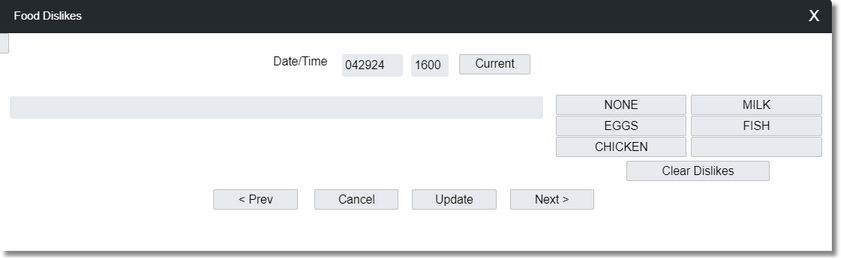
1.To document the patient's food dislikes, select the Food Dislikes question.
NOTE: A patient's food dislikes will display in the answer box, if previously documented in the Food Dislikes field, on the Patient Demographics - Encounter screen.
Food Dislikes
2.The Date/Time fields default to the current date and time. Modify these fields, if necessary.
3.Select the patient's food dislikes from the predefined options on the right side of the screen or enter the food dislike in the text box.
4.Select Next to save the information and advance to the next question, Update to save the information and return to the flow chart, Cancel to clear the entry and return to the flow chart, or Prev to save the information and go to the previous question.
NOTE: Food dislikes charted on this question will display in the Food Dislikes field on the Patient Demographics - Encounter screen.
Allergies
1.When the allergies question is selected, the user is taken to the Allergies application to review and update the patient's allergies. Please refer to the Allergies User Guide for detailed instructions on reviewing and updating a patient's allergies.
2.To return to the flow chart, select the blue back arrow.
Home Medications
1.When the home medications question is selected, the user is taken to the Medication Reconciliation application to review and update the patient's home medications. Please refer to the Medication Reconciliation User Guide for detailed instructions on updating a patient's home medications and completing medication reconciliation.
2.To return to the flow chart, select the blue back arrow.
Family Health History
1.When the family health history question is selected, the user is taken to the Health History application where they can review and update the patient's Family History, Functional/Cognitive Status, Health Concerns, Implantable Devices, Medical History, Social History, Referral/Transition of Care, Address History, Surgical/Procedural History, and Interventions. Please refer to the Health History User Guide for detailed instructions on reviewing and updating a patient's health history.
2.To return to the flow chart, select the blue back arrow.
Populating Questions/Answers to 24 Hour Summary and Patient Summary Reports
Questions set up to populate the question and answer information to the Health History section of the 24 Hour Summary and Patient Summary Reports will function as any standard question.